The Federal Government has just released the modelling behind its response to the COVID-19 pandemic. The modelling is theoretical and based on overseas data. Australia’s Chief Medical Officer Dr Brendan Murphy said this should not be considered predictive of Australia’s results, but covers three scenarios: an unmitigated scenario (uncontrolled spread), a scenario where we practice quarantine and self-isolation, and a scenario where we practice quarantine, self-isolation and social distancing measures. Tasmanian Times sought comments from a number of medical experts.
Professor Annette Dobson AM is a Professor of Biostatistics at the University of Queensland and Director of the Australian Longitudinal Study on Women’s Health.
“This is exactly what the Australian community asked for – modelling done by highly competent researchers, with all methods and assumptions clearly specified.
As the government’s summary points out, the modelling does not say what will happen but rather what could happen under various scenarios.
These early results are based on data from other countries. They will be updated using Australian data as the epidemic evolves. They should provide an excellent planning tool for Federal and State/Territory governments to tailor their responses over the coming months.”
——–
Professor David Wilson is the Head of Infectious Disease Modelling at the Burnet Institute
“It is striking how there is no fitting to any epidemiological data in Australia. This is astoundingly disappointing. They also only looked at a 25 per cent or 33 per cent reduction in social contacts. I don’t know why they aren’t looking at data from Facebook or Google (which was released recently) or elsewhere which suggest there are already considerably greater reductions in contact.
So, unfortunately, I do not find the projections to be realistic. There is no concern with the theoretical underpinnings – all very standard – and the qualitative conclusions are obvious about how the curve can be flattened and mitigated. But I do not find this satisfying for health system planning.”
——–
Professor Mikhail Prokopenko is Director of Complex Systems, Faculty of Engineering, University of Sydney. He recently modelled the pandemic in Australia.
“The Federal Government’s sharing of COVID-19 modelling is a welcome move. Not only will it allow the public to better understand the government’s decision-making process, but it will also allow experts to analyse the model, and provide their own recommendations in order to better hone the policy response to this ever-changing situation.
The Government’s model is mostly based on international data, not Australian data, while we calibrated our epidemic model specifically to Australian demographics and mobility data. Unlike our study, the Government’s model is coarse-grained, and does not include detailed predictions of what will actually occur in Australia.
The government’s future modelling plans include real-world Australian data – this would, of course, be a promising development, and we are looking forward to comparing these future extensions with the results which we have already developed by correlating our model with actual data.”
——–
Professor Nikolai Petrovsky, is a Professor in the College of Medicine and Public Health at Flinders University. He is also Research Director, Vaxine Pty Ltd
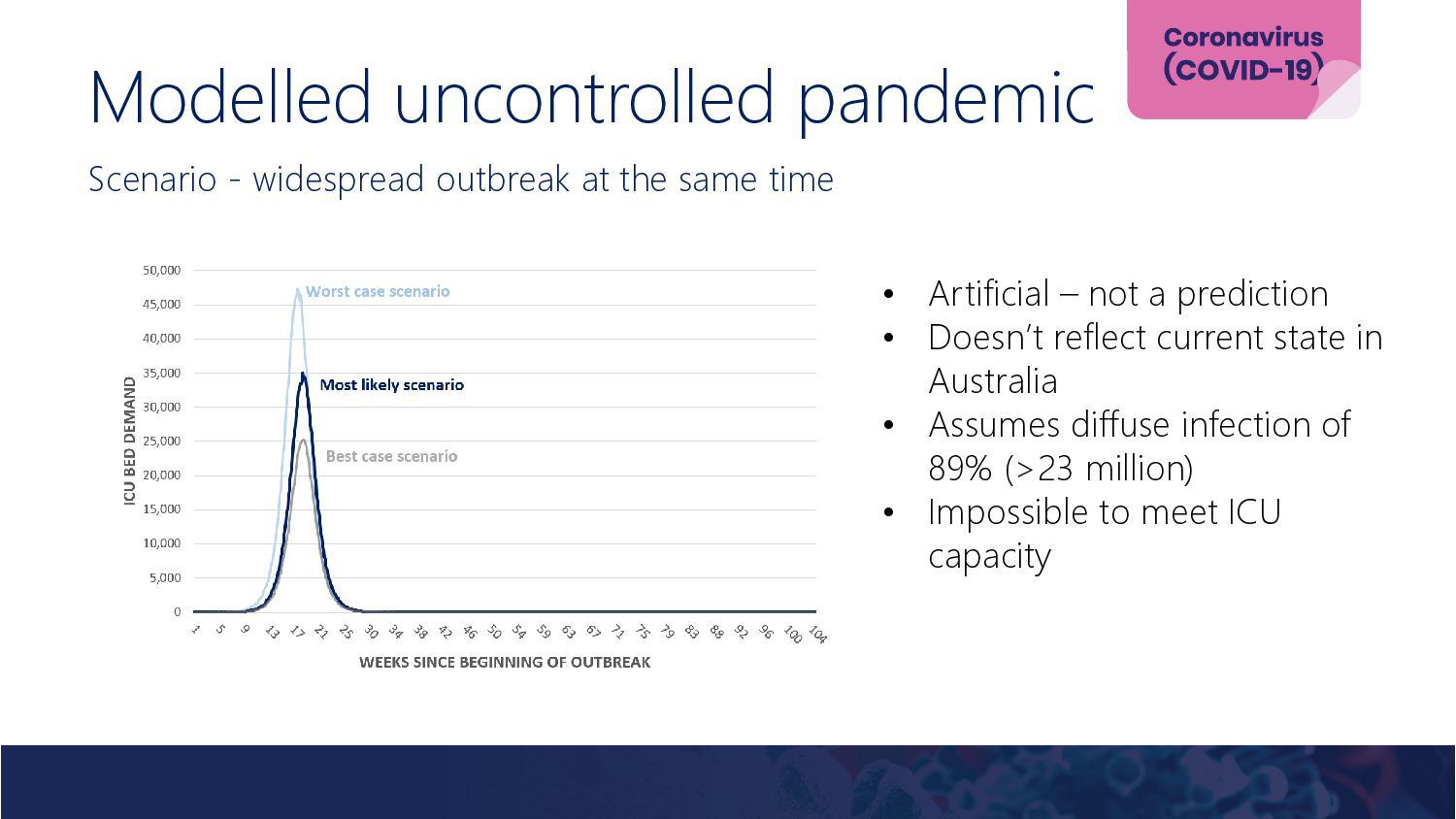
 “The key finding of the report is that ‘an unmitigated COVID-19 epidemic would dramatically exceed the capacity of the Australian health system, over a prolonged period’. Prolonged is the keyword as previously there has been the common perception based on 1908 pandemic influenza outbreak from US cities that the peak infection wave would complete in 2-3 weeks, causing a sharp peak in cases and mortality then rapid decline in cases as herd immunity was achieved.
“The key finding of the report is that ‘an unmitigated COVID-19 epidemic would dramatically exceed the capacity of the Australian health system, over a prolonged period’. Prolonged is the keyword as previously there has been the common perception based on 1908 pandemic influenza outbreak from US cities that the peak infection wave would complete in 2-3 weeks, causing a sharp peak in cases and mortality then rapid decline in cases as herd immunity was achieved.
This erroneous comparison led many politicians particularly in Italy, UK, Sweden and US to believe that all they needed to do was to let the COVID-19 sweep through the community, withstand a few weeks of excess hospital caseload and then the number of cases would rapidly fall due to herd immunity and hence the economy would quickly return to normal.
This belief that nothing needed to be done and the impact would only be temporary was completely unfounded, the problem being that too many commentators were making incorrect comparisons between COVID-19, a coronavirus, and influenza which is from the Orthomyxoviridae family. Although both cause respiratory infections that is where the similarity ends.
Hence, COVID-19 was never the equivalent of seasonal or pandemic influenza. It binds different receptors in the body, infects different cells and has different disease course.
Furthermore whilst human populations have a high level of background immunity to seasonal influenza strains and even potentially to pandemic influenza strains as highlighted by the many people who had innate protection to the 2009 swine flu pandemic virus, no humans have been shown to have immunity to COVID-19. This fact alone together with its different infectivity and disease course means that COVID-19 should never have been expected to behave like a seasonal influenza virus. Instead, any extrapolations should have been made based on the behaviour of its closest known relative, SARS coronavirus. In effect, COVID-19 is a more infectious, just slightly less lethal variant of SARS coronavirus. SARS did not go away spontaneously it was controlled by intense contact tracing, isolation and quarantine so that it was left with no opportunity to spread in the human population. The same might have worked for COVID-19 if it has been applied early enough. Now however it is well entrenched and as shown by this modelling might be possible to control but not eradicate by increasing physical isolation and reducing close person to person contact required for efficient transmission.
The fact that COVID-19 is not possible to eradicate by comparison to SARS, is that transmission of COVID-19 is possible from otherwise asymptomatic carriers, so that only intense contract tracing of every case combined with quarantine of all potential contacts, could hope to completely break its transmission, an activity most governments other than China have backed away from due to the enormous manpower resources required to do this successfully. So this report rightly models what happens if we accept that COVID-19 cannot be eradicated from the Australian population. In this scenario the virus will keep circulating and causing infections and fatalities. In order to not overload hospitals and ICUs the rate of infections need to be controlled, which the model shows can be achieved by increasing social separation. As the virus is not eradicated, not surprisingly as soon as this measure is relaxed, virus transmission increases and the case load again spikes to unmanageable levels.
The only conclusion which this report does not address is that without an effective vaccine, the only strategy to prevent hospital overload is to apply long term social separation. Eventually, once the majority of the people in the population have been infected, herd immunity will be established and social separation discontinued – how long would this take? If we assume a reason Australian case load would be 1,000 infections per day, then with a population of 24.6 million, it would take 24,600 days before everyone was infected. To achieve 85% exposure likely required for herd immunity, would take 20,910 days = 57 years. If we controlled the rate to 10,000 infections per day in Australia then it would still take 5.7 years. This is why the whole concept of easily achieving herd immunity was always completely spurious, and would mean accepting over 60 million deaths globally and 250,000 deaths just in Australia.
Hence, the only available conceivable strategy to achieve herd immunity more rapidly and thereby avoid the need for long-term social isolation is an effective COVID-19 vaccine, which is the current focus of the Vaxine research team based in Adelaide.”
Nikolai’s conflict of interest statement: Vaxine Pty Ltd has a COVID-19 vaccine in advanced preclinical development that is anticipated to commence human clinical trials in the near future.
——–
Associate Professor Hassan Vally is an epidemiologist with experience in infectious disease epidemiology, foodborne disease research, nutrition, child health, asthma and Indigenous Health.
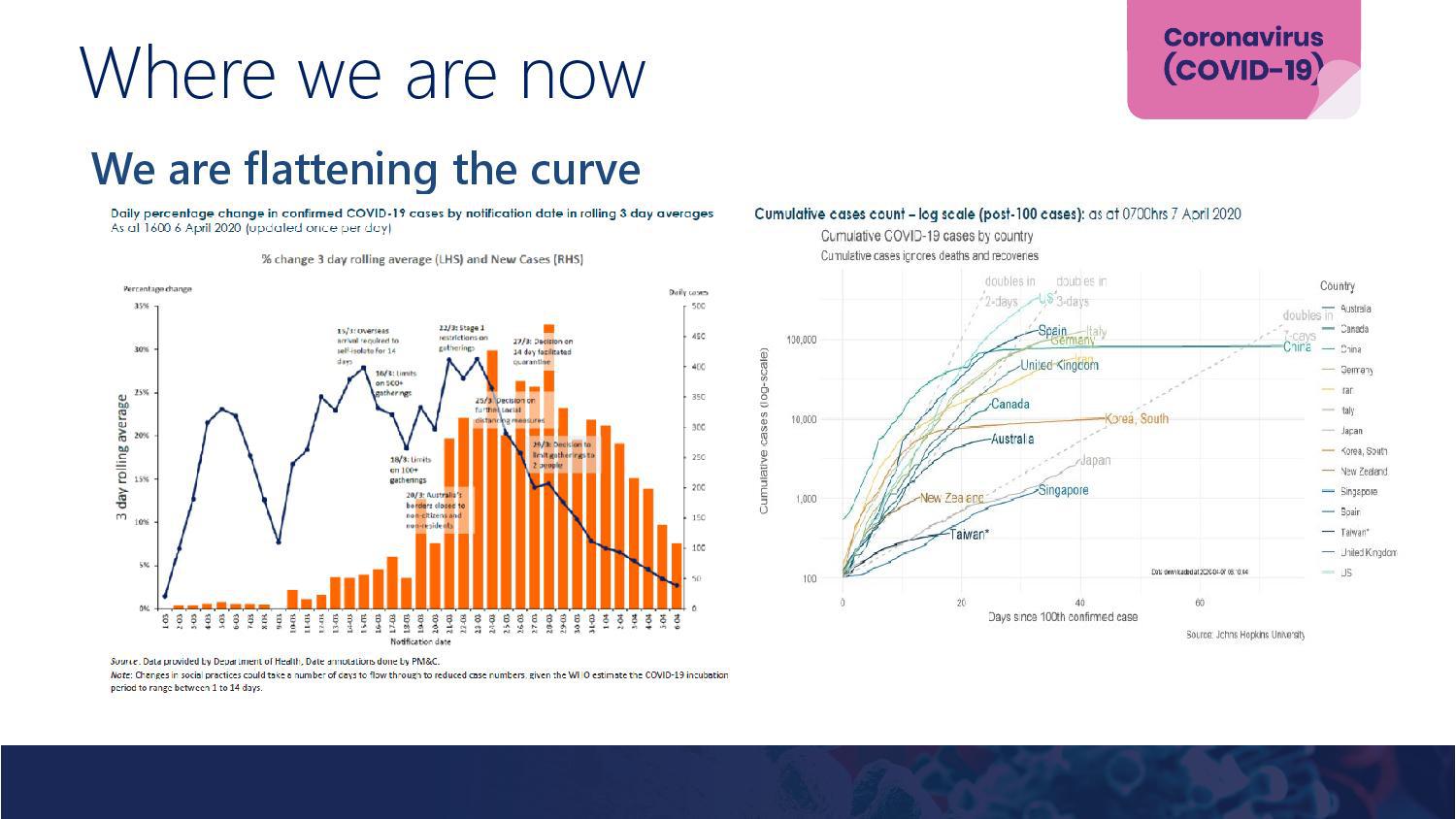
“It is really important to finally see the government modelling so that the Australian people can see the data that has been informing the decisions made during the pandemic. Having said that, there are few surprises here. It confirms what we have all understood that the more we do to try and slow the spread of the virus the further we flatten the curve and the extra time we buy as delay the peak of the pandemic.
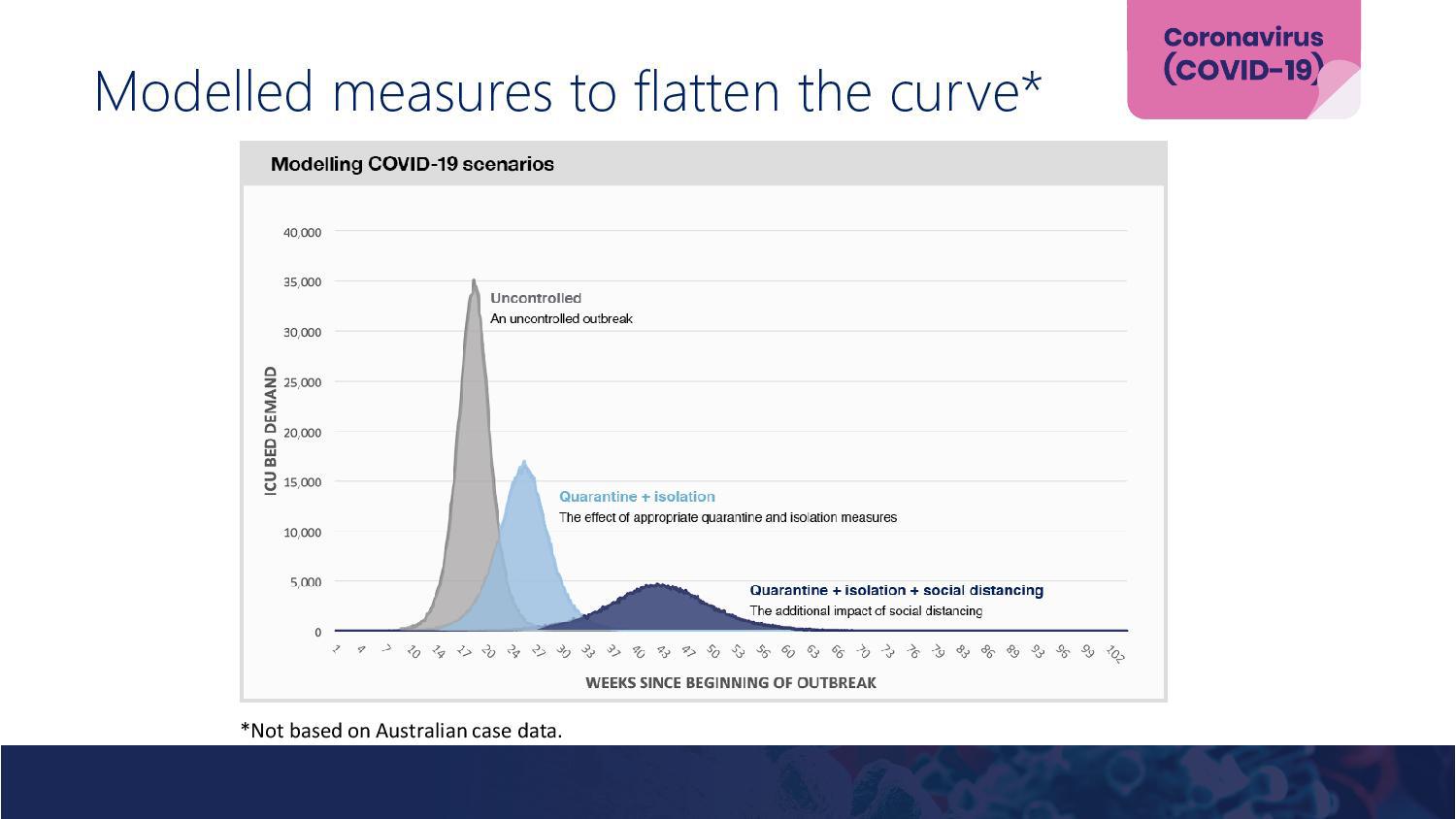
In terms of the specifics here, we see that if had been no response, we would see the peak of the pandemic occurring at around 17 weeks (just over 4 months) after the first case – which was in late January. This would have the peak occurring in May and would require the availability of 35,000 ICU beds. This would clearly be a public health disaster.
Instituting the public health measures of isolating cases and the quarantining of contacts, would see the peak delayed by another 7 weeks (almost 2 months) and would mean that the pandemic would peak in July and would require the availability of about half the number of beds that the uncontrolled pandemic would require. This is still an unmanageable situation.
The full mitigation scenario which includes isolation of cases, quarantining of contacts and social distancing delays the peak of the pandemic by another 19 weeks (approximately 5 months), so that it peaks in November. In this scenario, the peak of the pandemic requires the availability of about 14% of the number of ICU beds that would have been needed if there had been no mitigation strategies implemented. This is a significant reduction in the demand on the health system.
The upshot of this is modelling is that we are expecting the peak of the pandemic occurring approximately 7 months from now and so we should be expecting, as the government has signalled, for restrictions to be in place for at least that time and probably for a period after this.
It is really important with all modelling to be clear about the limitations in the data and the assumptions made. The government’s models are clear about the limitations which is good to see. The biggest limitations are that they have based their modelling on overseas data and also they have not taken into account the nuances of how the pandemic has evolved in Australia. Specifically, the fact that we have had a large proportion of cases linked to a few clusters.
It is clear, however, that this model will need to be updated and refined as we get more Australian data and this has also been highlighted in the release.
The biggest source of uncertainty in these predictions is the one that is most difficult to model and that is human behaviour. All of this highlights how much of a role society has in influencing the outcome of this pandemic.”
——–
Dr Alex Polyakov is a Senior Lecturer in the Department of Obstetrics and Gynaecology at The University of Melbourne and a Consultant Obstetrician, Gynaecologist and Fertility Specialist at the Reproductive Biology Unit at the Royal Women’s Hospital in Melbourne.
“There are a number of modelling techniques that may be utilised. The aim is to attempt to predict how the pandemic would unfold in Australia, so that the government may institute timely measures to mitigate its impact, try to initiate strategies to deal with its consequences and asses the possible long-term impact on the health system and the economy.
All models begin with initial assumptions which include a number of factors which can broadly be divided into inherent characteristics of the virus, characteristics of the population at risk of contracting the virus and possible outcomes in infected individuals. All these factors are important and some of them are largely unknown in regards to COVID-19. These initial assumptions are of paramount importance, as even small variations in characteristics that serve as model inputs may be magnified during the modelling process to arrive in extremely divergent outcomes. This is termed the ‘butterfly effect’ since there is sensitive dependence on initial conditions where a small change in one condition may result in large differences in the model’s outcome. This is reflected in wide confidence intervals of the final output of all models.
The situation can be compared to weather prediction modelling. Based on inputs from today it is possible to predict tomorrow’s weather with a high degree of certainty. On the other hand, the forecast becomes less and less certain as one tries to predict further into the future. The prediction for next Tuesday will be less accurate than for tomorrow and any attempt to predict the chance of rain on the 24th of May (as an example) will be largely meaningless without taking into account historical data accumulated over many years. One of the issues with the COVID-19 pandemic is that there is no precedent that we can turn to in order to improve modelling, except looking at countries that appear to be further into the pandemic compared to Australia. Unfortunately, every country is unique in terms of its population density, climate, ‘closeness’ of social interactions and actions taken in response to the pandemic threat. This explains the wide variation in infection and mortality rates between countries.
The first step in any modelling would be to attempt to predict the shape of the epidemic curve. How steep is the ascending portion? How high is the peak? These questions must be answered first in order to estimate the impact of the epidemic on the health system resources. Then assumptions will need to be made as to what proportion of the infected individuals will require medical interventions and how extensive those interventions will need to be. Taking into account all the assumptions that need to be made, it is clear that any conclusions that can be derived from various models must have a very high degree of uncertainty. At the same time it must be stressed that various changes in population behaviour as well as other, less defined factors, may also have a substantial and disproportionate impact on models outcomes.
An interesting and very simple exercise to demonstrate the above points can be performed on a standard Excel spreadsheet. Let’s assume that on day 1 there are 100 infected individuals. The number of infected individuals increases by a set percentage every subsequent day (this is termed geometric progression). This describes the ascending portion of the epidemic curve reasonably well. Let us then look at 5 per cent, 15 per cent and 30 per cent daily increase in the number of infected individuals for the next 30 days. When 5 per cent daily increase is applied, there are 412 infected individuals on day 30, a manageable number for almost any healthcare system. If the rate of increase is 15 per cent, the number on day 30 will rise to 5,858 individuals. Also manageable but may put some systems under stress. Most people are surprised to discover that if the rate of infection spread is 30 per cent per day for 30 days, there will be 201,538 infected individuals on day 30. No healthcare system in the world is able to cope with such a wave of patients. This exercise if awfully imprecise but demonstrates the uncertainties inherent in any modelling as well as the importance of flattening the curve to allow medical services to cope. The idea is to decrease the rate of new infections as much as possible. The good news is that in Australia the rate of newly diagnosed infections has been under 5 per cent for the past few days, unlike two weeks ago, when it approached 30 per cent.”

——–
Professor Sally Cripps is the Director of the Centre for Translational Data Science at the University of Sydney.
“Never has it been more important to have timely and high quality data. Modelling the spread of any disease is difficult, modelling the spread of an unencountered disease is impossible without real-time updating as data becomes available.
This is how science works, we build models, test these models against data and then update. This process usually takes years, for COVID-19 we need to do this in weeks.”
——–
Professor John Quiggin is an Australian Laureate Fellow in Economics at the University of Queensland.
“The idea of ‘flattening the curve’ is fundamentally misleading, since it implies that most people will be infected until herd immunity is achieved, while the number of cases remains within the capacity of the health system. But assuming spare capacity of 2 beds per 1000 people, and 20 per cent of patients requiring treatment, we would need at least five years for herd immunity to be achieved.
Optimal policy is to aim for near-complete eradication, then maintain sufficient distancing to ensure local outbreaks don’t spread. We will need quarantine for international arrivals until vaccination is general, or until other countries achieve near-complete eradication.
The main insight from economics is derived from the option value concept. Better to adopt stringent measures early and relax if they turn out to be excessive than to move slowly and risk widespread community transmission.”
——–
Dr Daswin De Silva is Deputy Director of the Centre for Data Analytics and Cognition (CDAC) at La Trobe University.
“This modelling exercise on international data is mostly retrospective, as it attempts to establish a correlation between current emergency response measures (quarantine and isolation, and social distancing) and the demand for critical medical care (ICU beds).
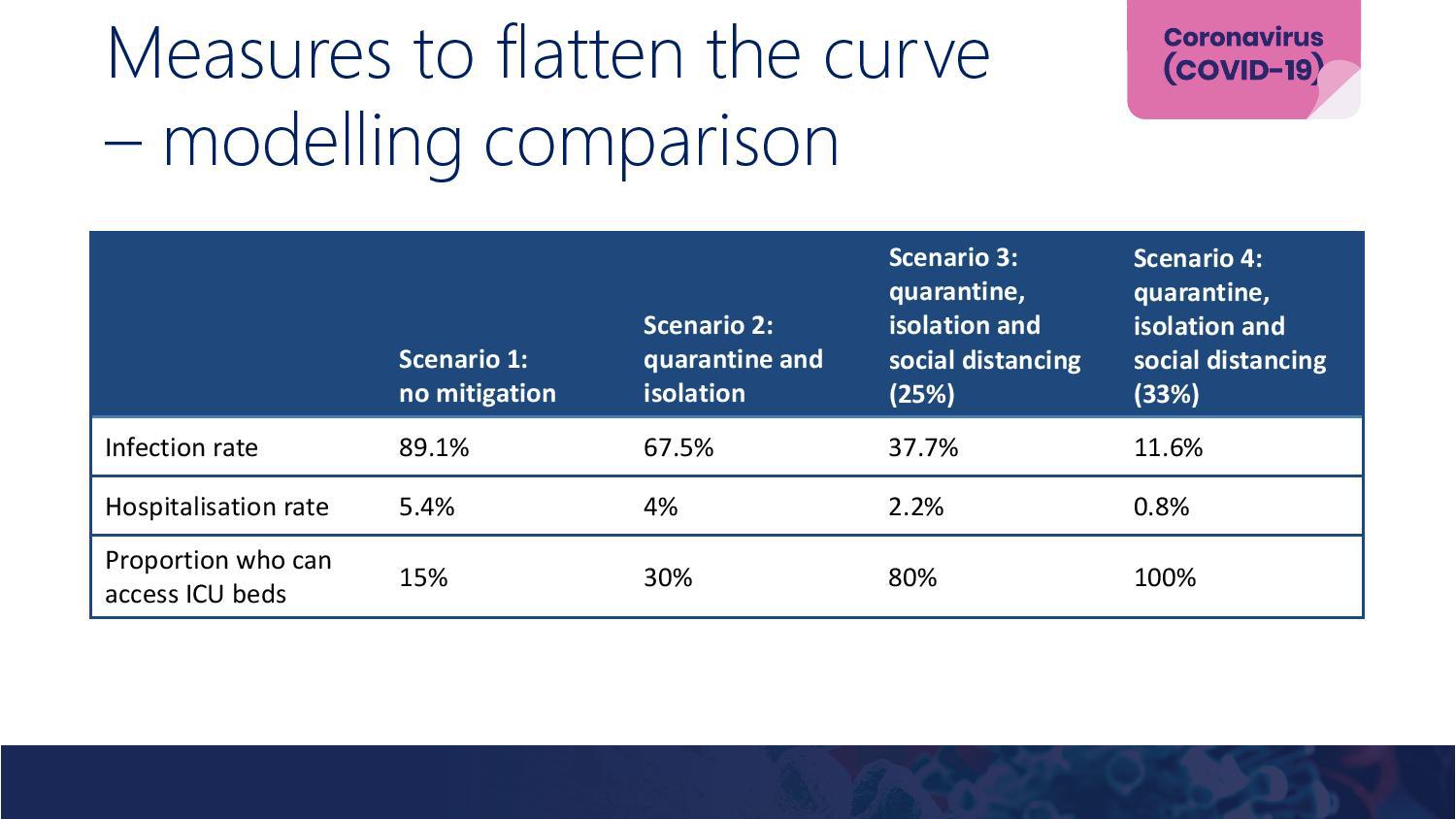
When evaluating the impact of emergency response measures, quarantine and isolation are bundled together possibly due to a lack of data to separate the two, and social distancing is presented as the most effective, accounting for two-thirds reduction of the intermediate peak.
In practice though, the implementation of these measures has not been as consistent, over time, across all states. This means the flattened curves will not be as smooth as depicted here.
By modelling exclusively for a single variable, ICU beds, it is assumed to be the single point of failure of our healthcare systems. Our reality is slightly different – as it disregards the potential impact of infections among doctors and nurses within a healthcare setting, such as the recently reported COVID-19 cluster at the Alfred.
The probability of a subsequent peak(s) has also been excluded in this modelling exercise. The single variable of ICU capacity will be insufficient to gauge the impact of such an eventuality.
When the Australian data is eventually modelled, it is important to address the exclusions noted above, and account for the granularity of the data. This means a drill-down from country-wide to state-level, followed by local council and postcode. A drill-down will have further use in the quick identification of unknown clusters of community transmission, as well as more targeted public health messaging.
It is also necessary for the Australia model to consider the onset of winter and the impact influenza on ICU capacity – at least the impact of influenza is a known variable across all hospitals.”
——–
Professor Carol Bower is a Senior Principal Research Fellow at the Telethon Kids Institute investigating the causes and effects of birth defects
“The modelling provides valuable information on which to base public health and clinical approaches to managing COVID-19 infections in Australia. The models are largely based on estimates and assumptions from overseas. It will be important to resource the collection of data in Australia to feed into the modelling, particularly including information on pre-symptomatic and asymptomatic transmission of the virus in the general population.”
——–
Professor Peter Gething is Kerry Stokes Chair in Child Health and Professor in Epidemiology at Curtin University and Telethon Kids Institute
“These models gave vital big-picture information to inform government thinking at the early stage of the outbreak in Australia. Using data from other countries, whose outbreaks were more advanced, they demonstrated how bad could things could get here if no action is taken, the impact on the health system and, to avoid that fate, the necessity of social distancing alongside border restrictions, isolation and quarantine. Those measures were put in place and we’re beginning to see the benefits – the rate of spread is slowing.
Just like the pandemic itself, however, the science of COVID-19 modelling is moving incredibly quickly. We now have a wealth of additional data – both internationally and from Australia itself – giving a richer picture on how the disease behaves and the impact of the public health measures put in place. The questions, too, are evolving rapidly. While honing strategies to further slow transmission is essential, interest is beginning to turn to the exit strategy. If cases continue to fall, how and when can restrictions be eased back, even before a vaccine is available? Here too, models will have a key role to play, creating virtual populations where different strategies can be tested.”
















